✨
Key Takeaways
→
Patient Registration Comprehensive intake form captures essential medical history and current health status for new patients.
→
Clinical Efficiency Streamlines consultation process by gathering vital information before the appointment begins.
→
Safety Protocols Identifies allergies, medications, and risk factors to ensure safe treatment delivery.
→
Personalised Care Enables healthcare providers to tailor treatment approaches based on individual patient needs and circumstances.
What is a General Practice Intake?
A General Practice Intake form is a standardised patient registration document that serves as the foundation for establishing comprehensive healthcare records within a general practice setting. This essential clinical tool systematically collects detailed information about a patient's medical history, current health concerns, lifestyle factors, and administrative details necessary for effective healthcare delivery.
The form functions as a critical communication bridge between patients and healthcare providers, ensuring that vital medical information is accurately captured before the clinical consultation begins. Furthermore, it establishes important legal and administrative foundations for the patient-provider relationship, including consent for treatment and data processing requirements under current healthcare regulations.
How to use General Practice Intake?
Step 1: Download the General Practice Intake Form
First, access the General Practice Intake PDF document by downloading it from Pabau below. The form is designed to be printer-friendly and can be completed either electronically using PDF editing software or printed and completed by hand. Ensure you have the most current version of the form to capture all necessary information fields and comply with current clinical documentation standards.
Step 2: Patient Information Collection
Begin by collecting comprehensive demographic and contact information from the patient. This includes full name, date of birth, address, telephone numbers, emergency contact details, and insurance or NHS information. Verify the accuracy of all personal details as these form the basis for patient identification and communication throughout their care journey.
Step 3: Medical History Documentation
Systematically document the patient's complete medical history, including past surgeries, chronic conditions, hospitalisations, and significant illnesses. Record all current medications, dosages, and frequency of administration. Additionally, document any known allergies or adverse drug reactions, ensuring this critical safety information is prominently noted for clinical reference.
Step 4: Current Health Assessment
Capture details about the patient's current health concerns, symptoms, and reason for seeking medical attention. Include information about symptom duration, severity, and any factors that improve or worsen the condition. This section should also cover recent changes in health status and any ongoing treatments or interventions.
Step 5: Lifestyle and Social History
Document relevant lifestyle factors that may impact health outcomes, including smoking history, alcohol consumption, exercise habits, occupation, and living arrangements. Record family medical history for conditions that may have genetic components, as this information can influence screening recommendations and treatment decisions.
Step 6: Review and Clinical Integration
Thoroughly review all completed sections for accuracy and completeness before filing in the patient's medical record. Ensure that any red flags or urgent concerns are immediately highlighted for clinical attention. The completed form should be integrated into the practice's electronic health record system or physical filing system according to established protocols.
Who is General Practice Intake helpful for?
The General Practice Intake form is invaluable for general practitioners, family medicine physicians, and healthcare teams working in primary care settings. It serves as an essential tool for nurse practitioners, physician assistants, and practice managers who need to establish comprehensive patient records and ensure continuity of care across multiple healthcare providers.
However, the form is equally beneficial for patients themselves, as it provides a structured opportunity to reflect on and organise their health information before meeting with their healthcare provider. This preparation enhances the quality of the consultation and ensures that important medical details are not overlooked during the appointment. Additionally, practice administrators and clinical staff find this form crucial for maintaining accurate patient databases and supporting quality improvement initiatives within the healthcare facility.
Benefits of using General Practice Intake
The implementation of a comprehensive General Practice Intake form offers numerous advantages for both healthcare providers and patients:
- Enhanced clinical efficiency through systematic information gathering before consultation begins
- Improved patient safety by identifying allergies, drug interactions, and contraindications early
- Better care coordination through comprehensive documentation of medical history and current treatments
- Reduced consultation time wastage, allowing more focused discussion of current health concerns
- Strengthened medicolegal protection through thorough documentation and informed consent processes
The systematic use of this intake form creates a solid foundation for evidence-based healthcare delivery whilst ensuring that both clinical and administrative requirements are met from the outset of the patient relationship.
Legal and Regulatory Considerations
General Practice Intake forms must comply with current data protection regulations, including GDPR requirements for patient consent and data processing. The form should clearly outline how patient information will be used, stored, and shared within the healthcare team. Additionally, practices must ensure that completed forms are securely stored and that access is restricted to authorised healthcare personnel only.
It's essential that the intake process includes appropriate consent mechanisms for treatment, data sharing with other healthcare providers, and communication preferences. The form should also address patient rights regarding access to their medical records and procedures for updating or correcting information as circumstances change.
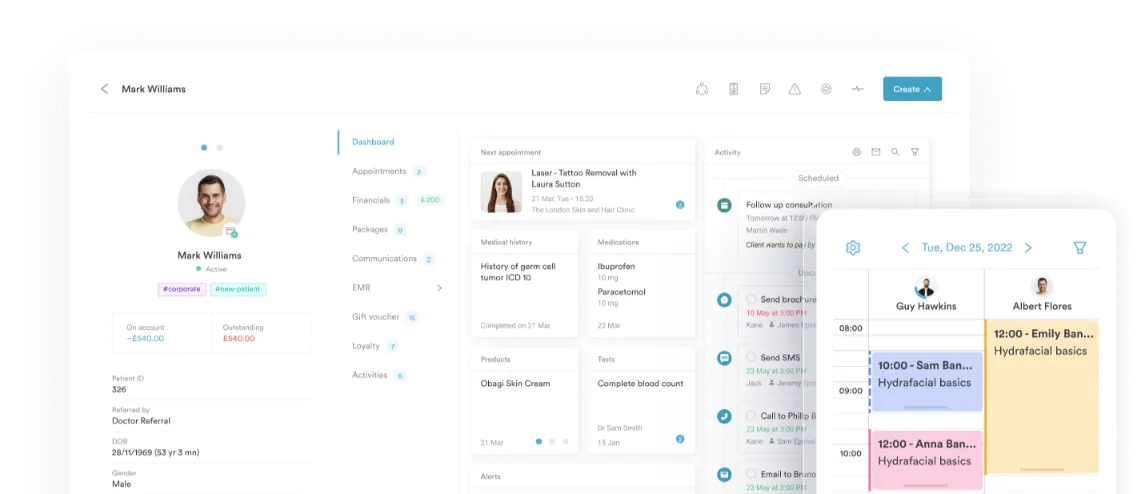
Digital Integration and Modern Practice Management
Contemporary general practices increasingly integrate intake forms with electronic health record systems and practice management software. This digital approach enables automatic population of patient databases, reduces transcription errors, and facilitates seamless information sharing between different healthcare providers within the same organisation.
Digital intake systems can also include automated alerts for important clinical information such as allergies or chronic conditions, enhancing patient safety protocols. Furthermore, electronic forms can be completed by patients prior to their appointment through patient portals, improving practice efficiency and reducing waiting room congestion whilst maintaining comprehensive documentation standards.
PDF Template
General Practice Intake
Frequently asked questions
What information should be included in a General Practice Intake form?
A comprehensive General Practice Intake form should include demographic details, complete medical history, current medications and allergies, family history, lifestyle factors, current symptoms, emergency contact information, and consent for treatment and data processing.
How long should patients spend completing the General Practice Intake form?
Patients should allow approximately 15-20 minutes to complete a thorough General Practice Intake form, though this may vary depending on the complexity of their medical history and current health concerns.
When should the General Practice Intake form be updated?
The intake information should be reviewed and updated at least annually during routine appointments, whenever there are significant changes in health status, medications, or personal circumstances, and following any hospitalisations or specialist consultations.
What are the legal requirements for storing General Practice Intake forms?
Intake forms must be stored securely in compliance with GDPR and healthcare record retention policies, with access restricted to authorised personnel, and retained for the required period as specified by medical record keeping guidelines.
Can General Practice Intake forms be completed electronically?
Yes, many practices now offer electronic intake forms through patient portals or digital platforms, which can improve accuracy, reduce processing time, and integrate seamlessly with electronic health record systems.
How does the General Practice Intake form improve patient safety?
The form enhances patient safety by systematically capturing allergies, drug interactions, contraindications, and risk factors before treatment begins, enabling healthcare providers to make informed decisions and avoid adverse events.